Aetna Medicare Appeal Form
Or a Medicare Part B prescription drug you have the right to ask us for an appeal of our decision. State-specific forms about disputes and appeals.
Fillable Online Aetna Appeal Form Fax Email Print Pdffiller
Aetna Medicare Part C Appeals Grievances PO Box 14067.
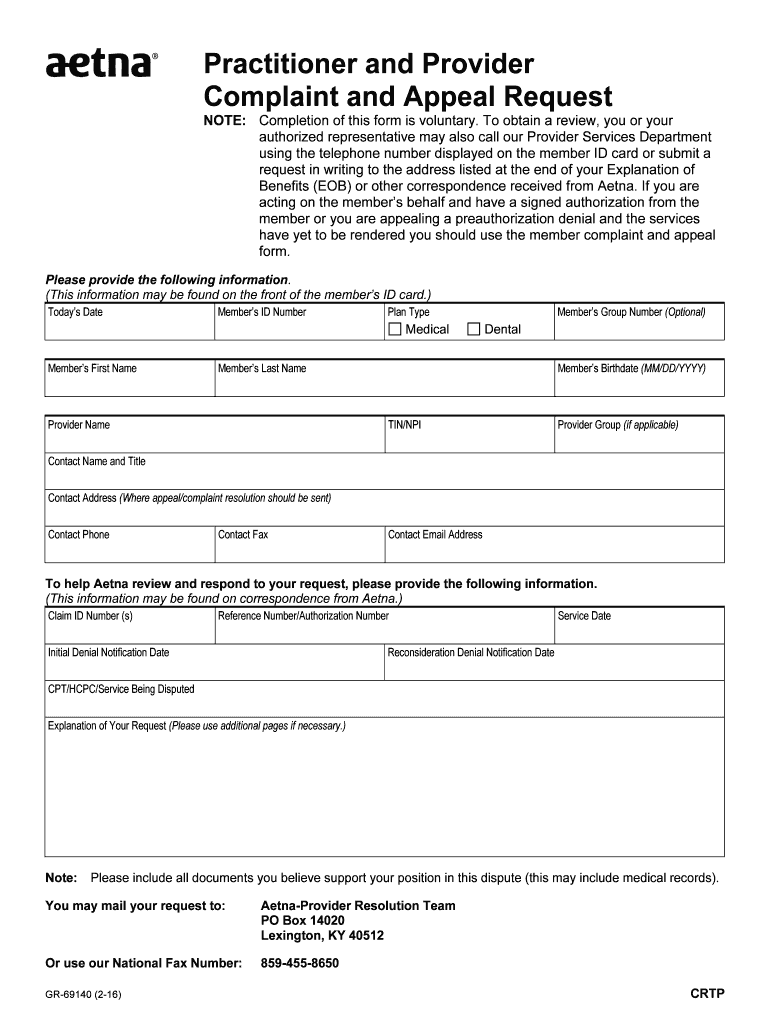
Aetna medicare appeal form. Aetna-Provider Resolution Team PO Box 14020 Lexington KY 40512. You may mail your request to. Non-PAR Provider Appeal form Medicare-Medicaid Coverage determination online Medicare-Medicaid Plan Pharmacy Provider Pharmacy Coverage Determination form Medicare-Medicaid Plan Pharmacy updated 4142021.
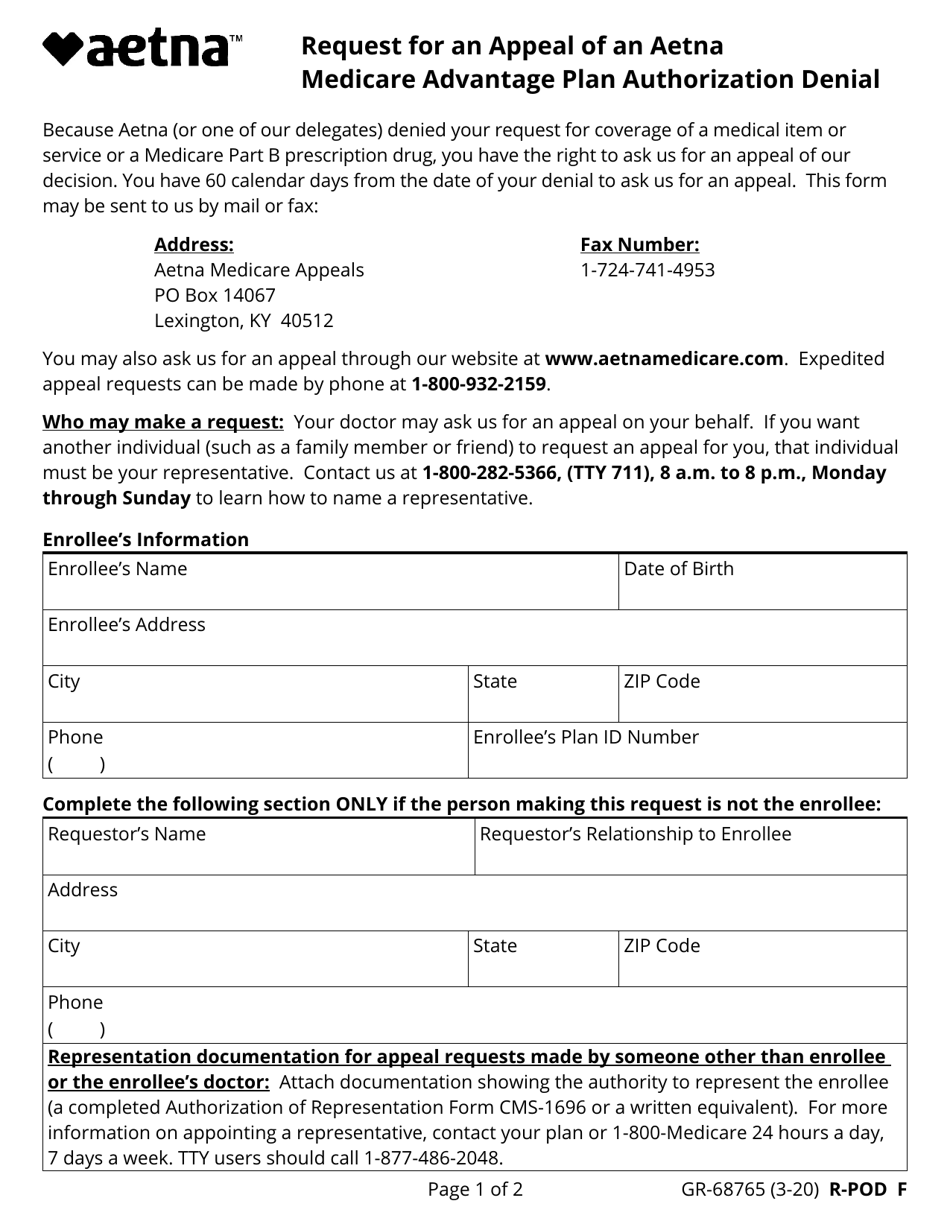
Expedited appeal requests can be made by phone at 1. Box 14067 Lexington KY 40512 Telephone. Print an authorization appeal form Fax.
You cannot request an expedited appeal if you are asking us to pay you back for a drug that you already received. This form may be sent to us by mail or fax. We have state-specific information about disputes and appeals.
Aetna Medicare Appeals PO Box 14067 Lexington KY 40512. Start a free trial now to save yourself time and money. If you are an Employer Group Medicare Advantage member please use the below forms.
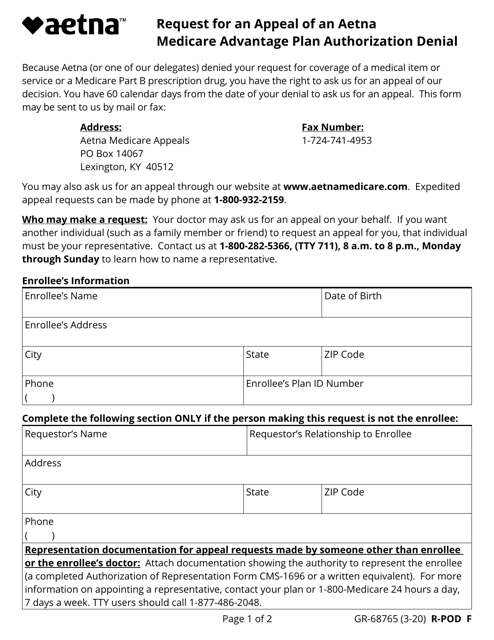
What To Do When a Loved One Passes Away. You have 60 calendar days from the date of your denial to ask us for an appeal. Request for an Appeal of an Aetna Medicare Advantage Part C Plan Claim Denial.
Because Aetna or one of our delegates denied your request for payment for medical benefits you have the right to ask us for an appeal of our decision. Available for PC iOS and Android. Because Aetna Medicare or one of our delegates denied your request for payment of medical benefits you have the right to ask us for an appeal of our decision.
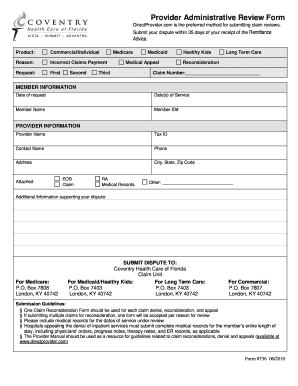
Payment appeals for Contracted provider requests. We also have a list of state exceptions to our 180-day filing standard. Whether your spouse has just passed.
Aetna medicare appeal form. This form may be sent to us by mail or fax. Or use our National Fax Number.
Aetna Medicare Part C Appeals PO Box 14067 Lexington KY 40512 If you need a faster expedited decision you can call or fax us. Expedited appeal requests can be made by phone at 1-877-235-3755 TTY. Exceptions apply to members covered under fully insured plans.
WAIVER OF LIABILITY STATEMENT. Get a Provider Complaint and Appeal form PDF Timing and scope of changes As of March 1 2017 the change affected all Aetna medical plans including Aetna Medicare plans. This form may be sent to us by mail or fax.
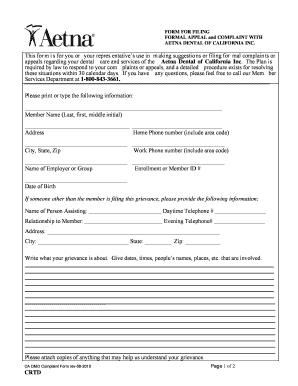
Aetna Medicare is a PDP. Aetna Medicare Plans Complaint and Appeal Form This form is for your use in making suggestions filing a formal complaint grievance or appeal regarding any aspect of the service provided to you. You have 60 days from the date of our Notice Denial of Medicare Prescription Drug Coverage to ask us for a redetermination.
Fill out securely sign print or email your Aetna Medicare Plans - Complaint and Appeal Form instantly with signNow. We are required by law to respond to your complaints or appeals and a detailed procedure exists for resolving these situations. You have 60 days from the date of our written denial notice to ask us for an appeal.
Please submit your appeal request with the fully completed form and any additional medical records notes or other documentation you would like reviewed with your request. This form may be sent to us by mail or fax. Please note that this is not a new requirement or process.
Pre-Service Post Service To help Aetna review and respond to your request please provide the following information. 711 7 days a week 24 hours a day. UAetna Medicare Prescription Drug Plan Aetna Medicare Grievance Appeals PO Box 14579 Lexington KY 40512.
You have 60 calendar days from the date of your denial to ask us for an appeal. Find the Aetna Medicare forms you need to help you get started with claims reimbursements Aetna Rx Home Delivery filing an appeal and more. If you have a dispute around the rate used for payment you have received please visit Health Care Professional Dispute and Appeal Process.
Please check the box to verify that you are the individual completing this form. State exceptions to filing standard. Aetna Appeal Form 2021.
Appealing a preauthorization denial and the services have yet to be rendered use the member complaint and appeal form. The most secure digital platform to get legally binding electronically signed documents in just a few seconds. This form may be sent to us by mail or fax.
Because Aetna Medicare denied your request for coverage of or payment for a prescription drug you have the right to ask us for a redetermination appeal of our decision. Expedited urgent and pre-service appeals are considered member appeals and are not affected. Keep a copy of everything you send to Medicare as part of your appeal.
Print a claim denial appeal form. Aetna Medicare Part D Appeals Grievances PO Box 14579 Lexington KY 40512. These changes do NOT affect member appeals.
If youre appointing someone to help with your appeal send the representative a form or written request with your appeal request to the Medicare Administrative Contractor MAC the company that handles claims for Medicare or your Medicare health plan. Because Aetna Medicare denied your request for coverage of or. To download Medicare appeal forms from the governments Medicare website click here.
This information may be found on correspondence from Aetna Claim ID Number If Post Service selected above Reference Number. UAetna Medicare Advantage Plan U Aetna Medicare Grievance Appeals PO Box 14067 Lexington KY 40512. You are now leaving Aetna Better Health of Michigans website.
06202013 ADVERTISEMENT Related Articles. You have 60 calendar days from the date of your denial to ask us for an appeal. 6 hours ago Aetna Medicare Appeals PO Box 14067 Lexington KY 40512.
Please advise if the appeal is related to. A completed Aetna Provider Complaint and Appeal form is required when submitting provider appeals. Authorized Representative Form with your request.
Because Aetna Medicare or one of our delegates denied your request for coverage of a medical item or service or a Medicare Part B prescription drug you have the right to ask us for an appeal of our decision.
Prescription Drug Plan Aetna Medicare
Fillable Online Aetna Appeal Form Fax Email Print Pdffiller
2
Form Gr 68765 Download Fillable Pdf Or Fill Online Request For An Appeal Of An Aetna Medicare Advantage Plan Authorization Denial Aetna Templateroller

Aetna Medicare Advantage Appeal Form Fill Online Printable Fillable Blank Pdffiller

Want To Know How To Write Effective And Stand Out Cvs Check It Out Worker Compensation Risk Management
2

Coverage Decisions Appeals And Grievances Aetna Medicare
Fillable Online Aetna Appeal Form Fax Email Print Pdffiller
Aetna Reconsideration Form 2021 Pdf Fill Out And Sign Printable Pdf Template Signnow
Aetna Member Complaint And Appeal Form Fill Online Printable Fillable Blank Pdffiller
2
2
Form Gr 68765 Download Fillable Pdf Or Fill Online Request For An Appeal Of An Aetna Medicare Advantage Plan Authorization Denial Aetna Templateroller
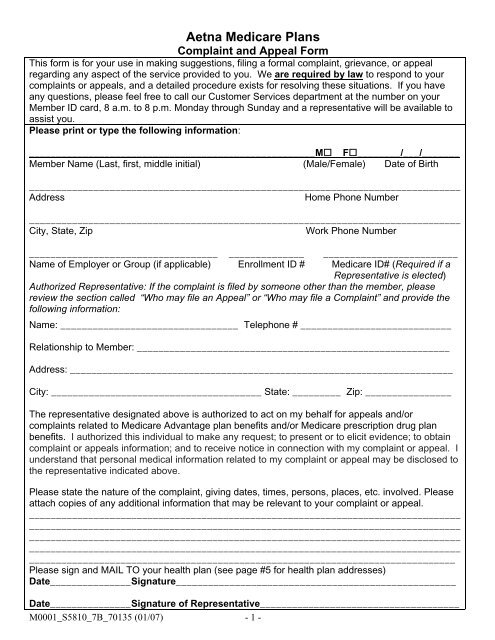
Aetna Medicare Plans Complaint And Appeal Form
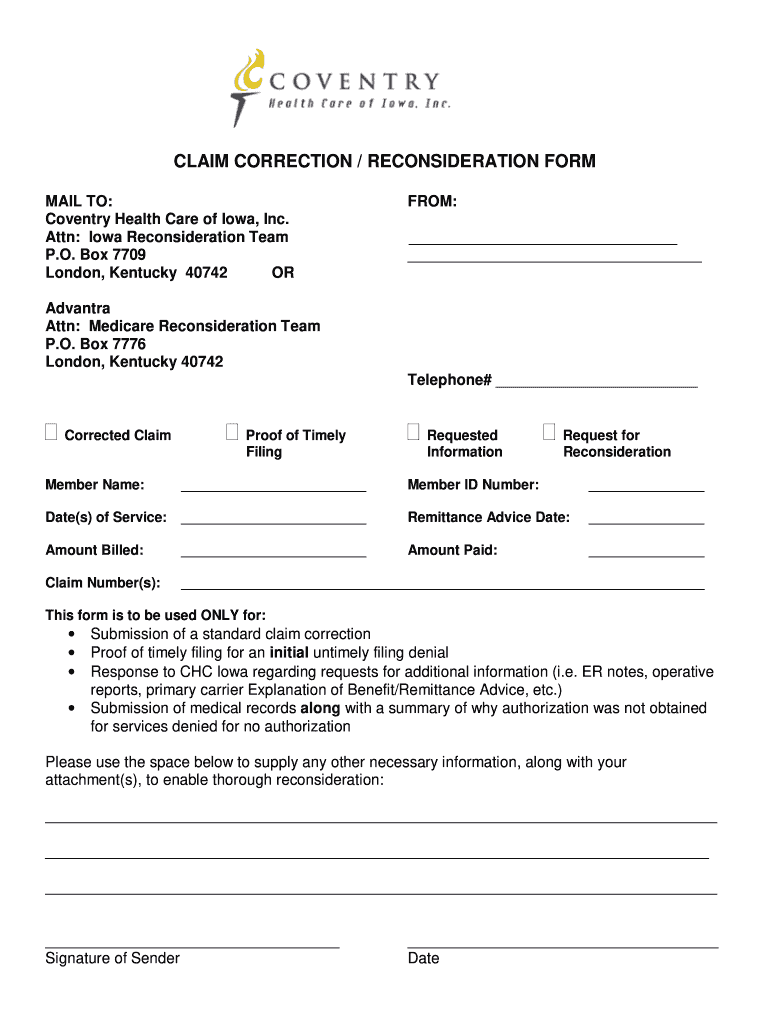
Coventry Advantra Provider Appeal Form Fill Online Printable Fillable Blank Pdffiller

Aetna Better Health Ohio Appeal Medicare Fill Online Printable Fillable Blank Pdffiller
Aetna Appeal Form 2021 Fill Out And Sign Printable Pdf Template Signnow
2
